



Infection control is a major priority within critical care. All our patients are highly susceptible to hospital acquired infection (HAI). Meticulous attention to HAND HYGIENE is the mainstay of preventing HAI.
Always wear an apron and gloves if you are within a patient bed area (i.e nearer than the observation chart/board). Visiting teams should also wear aprons. Please politely remind visiting teams e.g. surgeons if they are not wearing gloves and aprons in a bed space.
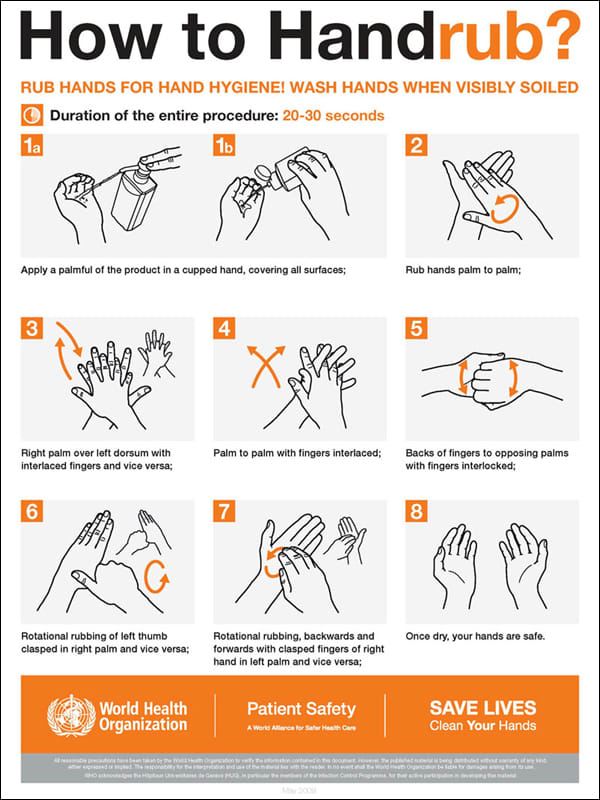
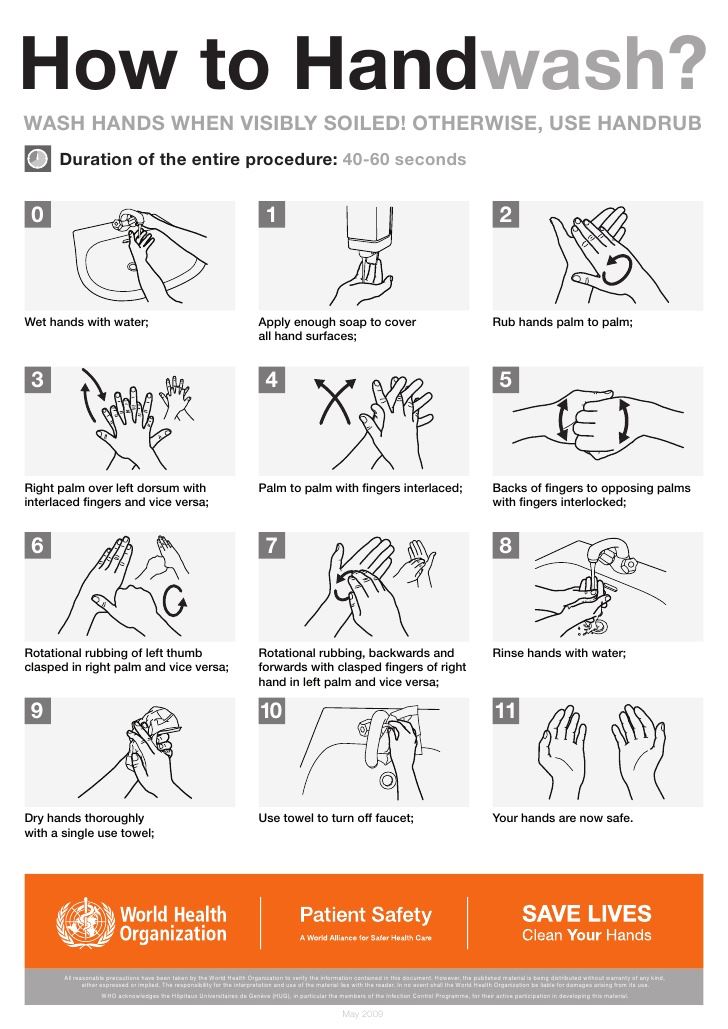
We comply with the ‘CleanYourHands’ campaign. You should clean your hands before and after every patient or notes contact. If hands are apparently clean then alcohol gel can be used. If hands are visibly contaminated then you must wash your hands at the sink.
Patient Isolation
There is a single isolation cubicle on each ICU and 3 isolation cubicles and 1 sideward on HDU. Patients with contagious infections e.g C Diff, MRSA, VRE, require barrier nursing in a cubicle to prevent spread to other patients. Immunosuppressed patients require reverse barrier nursing in a cubicle to protect them from pathogens. Discussion with the Consultant, Senior Nurse and Microbiology team are required if more than two patients within ICU require an isolation cubicle. Additional Personal Protective Equipment (PPE) may be necessary where appropriate (FFP3 mask etc).
Hand washing should be with soap and water for patients requiring isolation.
MRSA
All patients are screened for the presence of MRSA on admission to the unit. After swabs have been taken, all patients receive Octenisan skin wash (once daily) and Mupirocin nasal ointment (TDS) for a minimum of 5 days even if the swab results are all negative (usually available within 48 hours). Please document on the daily sheet if any patient is MRSA or C diff positive. If the patient was negative on admission then becomes positive it is unit acquired. If a patient is MRSA positive then please prescribe eradication therapy as directed by the infection control team.
C difficile
If a patient has been identified as having C diff should die whilst in Critical Care you must discuss with the Consultant in Charge before completing the Death Certificate. If the death is as a result of C diff infection, this needs to be discussed with Prof Bellamy, Consultant in Infectious Diseases.
Blood Cultures
Blood cultures should be sent via a ‘fresh’ peripheral blood sample. The site from which cultures are taken must be clearly labelled on the request form e.g. ‘from CVC line at time of insertion’ or ‘peripheral’. We are moving away from the practice of taking routine blood culture samples from arterial lines and central lines. If lines are thought to be the source of the sepsis then the line should be changed. Skin and/or ports used for taking samples must be thoroughly cleaned with Chlorhexidine prior to taking the sample to minimise the risk of contamination of specimen.
Equipment
If you use any equipment within a bed area e.g ultrasound machine / doppler then it must be cleaned with the appropriate cleaning solution / wipes before returning to the storage area. Please ask a Consultant, RGN or Health Care Assistant which cleaning solution is appropriate.
Invasive procedures
Meticulous aseptic technique should be observed at all times. You should use Hibiscrub, which is available at the ‘middle’ sink on each unit, for hand washing prior to invasive procedures. You should always wear a hat, mask, sterile gown and sterile gloves, use chlorhexidine skin prep (via the chloroprep ‘sticks’) and fully drape the patient for any invasive procedure (central lines, lumbar punctures, chest drains). Individual sterile drapes are always available should you require any extra to those that are provided. A chlorhexidine impregnated gelpad should be applied to all invasive lines underneath the clear adhesive dressing. See the guideline for practical procedures.
We have pre-printed documents for recording the skin preparation and insertion technique for central venous catheters and arterial lines. For CVC, there is a section for a witness to sign that the guidewire has been removed. Please ensure the document is given to the nursing staff who will monitor the skin insertion site and document line removal.
 ©General Critical Care STH 2025
©General Critical Care STH 2025